 فارسی
فارسی 
Abstract
The term LASER stands for “Light Amplification by the Stimulated Emission of Radiation”.
Since the first application of laser in dentistry by Miaman in 1960, this technology has been used in various fields of hard and soft tissue. In the last two decades, extensive research has been conducted in the field of laser applications.
In the field of hard tissue, lasers are used to prevent caries, whiten teeth, remove and harden restorative materials, prepare dental cavities, treat dentinal hypersensitivity, modulate growth, and also for diagnostic purposes.
In the field of soft tissue, lasers are also used in wound healing, remove hyperplastic tissues, expose impacted or partially erupted teeth, photodynamic therapy in malignancies, and stimulate herpetic lesions.
Laser application has proven to be an effective tool for increasing efficiency, accuracy, convenience, cost reduction and improving the comfort of dental treatments.
Diode laser has a significant advantage over other lasers by providing precise cuts in soft tissue with less bleeding and pain, as well as due to its lower cost and ease of maintenance.
Keywords: Dental applications, lasers, optical stimulation, diode laser
Introduction
The introduction of lasers into dentistry in the 1960s by Miaman [1] marked the beginning of continuous research on the diverse applications of lasers in dental treatments. There are two main approaches in this field:
On the one hand, hard lasers such as carbon dioxide (CO2), neodymium:yttrium-aluminum-garnet (Nd:YAG) and Er:YAG, which are used in both hard and soft tissues, but have limitations due to their high cost and the possibility of thermal damage to the dental pulp [2,3].
On the other hand, cold or soft lasers, which are based on semiconductor diode devices, are compact, low-cost devices that are mainly used for therapeutic applications. These lasers are generally known as low-level laser therapy (LLLT) or biostimulation [4].
Lasers are recommended for a wide range of treatments in dentistry due to their ease, efficiency, precision, convenience, and cost-effectiveness compared to conventional methods [5-8]. The aim of this review is to focus on the applications of lasers in hard and soft tissue in dentistry.
History
In 1917, Albert Einstein [9] laid the foundation for the invention of the laser and its prototype, the maser, by proposing a theory about the amplification of light that could lead to stimulated emission of a single frequency.
The term LASER, which stands for “Light Amplification by the Stimulated Emission of Radiation”, was first introduced to the public in a 1959 paper by Gordon Gould, a graduate student at Columbia University [10].
Theodore Miaman at Hughes Research Laboratories in Malibu, California, built the first practical laser using a mixture of helium and neon [1]. In 1961, a laser was developed using yttrium-aluminum-garnet crystals doped with 1 to 3% neodymium (Nd:YAG) [10].
In 1962, the argon laser was developed, and a year later, in 1963, the ruby laser was used as the first medical laser for coagulation of retinal lesions [10]. In 1964, Patel at Bell Laboratories developed the carbon dioxide (CO2) laser [10].
Today, diode lasers are widely used in dentistry.
Types of Lasers
Lasers used in dentistry can be classified in several ways:
Based on the laser medium used, such as gas and solid state lasers;
Based on the tissue application, including hard tissue and soft tissue lasers;
Based on the wavelength range [Figure 1];
And of course, based on the level of potential hazards associated with laser application.
Carbon Dioxide Laser (CO₂ Laser)
CO₂ lasers have a very high tendency to absorb water due to their wavelength. This feature allows for rapid soft tissue ablation and hemostasis (control of bleeding) with very shallow penetration.
Although this laser has the highest absorption rate [11] among all laser types, it also has disadvantages, including large size of the device, high cost, and destructive reactions in hard tissue. Also, the beam delivery medium in CO₂ lasers is often provided by mirror arms (waveguides), which, although allowing for precise beam guidance, increases the volume and complexity of the system.
Neodymium: Yttrium-Aluminum-Garnet Laser (Nd:YAG Laser)
The wavelength of the Nd:YAG laser is significantly absorbed by pigmented tissues, making it a very effective surgical laser for cutting and coagulation of dental soft tissue while providing adequate hemostasis.
In addition to surgical applications [12], research has also been conducted on the use of the Nd:YAG laser for non-surgical debridement of the gingival sulcus in the control of periodontal diseases [13] and also in the Laser Assisted New Attachment Procedure (LANAP) [14].
Erbium Laser
The erbium laser family has two distinct wavelengths:
Er, Cr: YSGG Yttrium-Scandium-Gallium-Garnet
Er:YAG Yttrium-Aluminum-Garnet
Erbium wavelengths have a high affinity for hydroxyapatite and also exhibit the highest water absorption of all wavelengths of dental lasers. For this reason, this class of lasers is considered the primary choice for the treatment of dental hard tissues [15].
In addition to their use in hard tissues, erbium lasers can also be used in soft tissue ablation, as oral soft tissues also contain a high percentage of water [16].
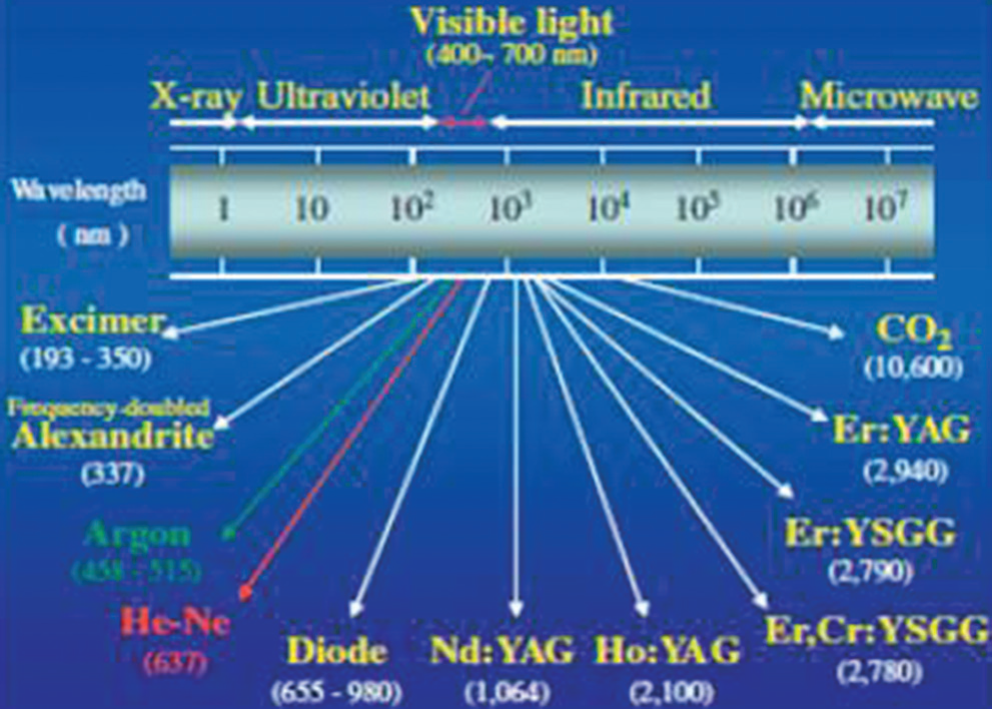
Figure 1: Different types of lasers and their corresponding wavelengths
Diode Laser
The diode laser is one of the most widely used lasers in modern dentistry, which is particularly popular due to its small size, high efficiency, and relatively affordable price. The active medium of this laser is a solid-state semiconductor made of aluminum, gallium, arsenide, and in some models, indium, and its wavelengths are in the range of approximately 810 to 980 nm. These wavelengths are designed to have the highest absorption by tissue pigments such as melanin and hemoglobin in the blood, while their absorption by hydroxyapatite in tooth enamel and tissue water is very low.
The high absorption characteristic of pigments and hemoglobin makes the diode laser an ideal tool for soft tissue applications in the mouth and gums. This laser is particularly useful in cosmetic gum surgery, increasing the length of the soft tissue dental crown and revealing impacted teeth in soft tissue. It can also be used to remove inflamed and hypertrophic tissues, perform frenectomies, and photostimulate aphthous and herpes lesions [17].
Recently, the 450 nm wavelength has entered the dental field as the newest wavelength applied in diode lasers. This shorter wavelength than the traditional 810–980 nm range offers very high absorption by hemoglobin and tissue pigments, which increases the precision of soft tissue cutting, effectively controls bleeding, and reduces thermal damage to surrounding tissues. The high hemoglobin absorption at this wavelength allows for precise and minimally invasive surgeries, such as excision of inflamed or hypertrophic tissue, frenectomy, and aesthetic gingival remodeling, and by improving hemostasis, reduces the duration of the procedure, and increases patient comfort. This scientific characteristic of the 450 nm wavelength makes it an efficient and safe tool for soft tissue surgical applications in modern dentistry.
In addition to surgical applications, the diode laser is considered a safe alternative to traditional soft tissue surgery methods in dentistry due to its good bleeding control, minimal thermal damage to surrounding tissues, and increased patient comfort. On the other hand, its use in photostimulation and tissue repair stimulation has led to its widespread use in conservative and cosmetic treatment protocols.
In short, the diode laser is a versatile, precise, and safe tool that can be used in both cosmetic and therapeutic surgeries as well as non-invasive procedures, and for this reason it is considered one of the most popular lasers in modern dentistry.
Laser Operation Mechanism
Laser light is monochromatic light, consisting of only one specific wavelength. The structure of a laser system consists of three main parts:
Energy source
Laser active medium
Two or more mirrors that form an optical cavity or optical resonator.
In order for the light to be amplified, energy is injected into the laser system through a pumping mechanism. This energy can be supplied from sources such as a flash lamp, an electric current, or an electric coil. The energy introduced into the active medium, which is located inside the optical resonator, causes the spontaneous emission of photons.
The amplification process then occurs through stimulated emission, in which photons are reflected back and forth in the active medium by the highly reflective surfaces of the resonator, increasing the light intensity. Finally, the photons are emitted through the output coupler of the resonator [Figure 2].
In dental lasers, laser light is transmitted to the target tissue via a fiber optic cable, hollow waveguide, or articulated arm [Table 1]. In addition, the laser system usually includes focusing lenses, a cooling system, and other controls to optimize performance and safety.
This mechanism allows the laser to focus light energy with high precision and in very limited tissue areas, providing excellent therapeutic efficacy in surgery and treatment of hard and soft dental tissues.
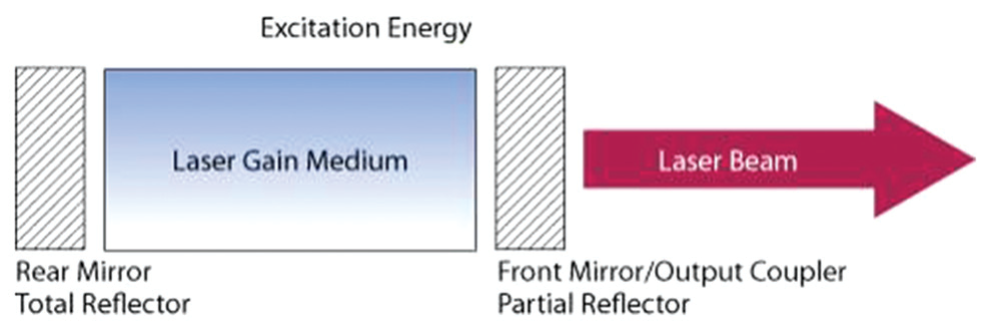
Figure 2: Laser operating mechanism
Table 1: Common types of lasers used in dentistry
| Laser Type | Structure | Wavelength (nm) | Light Delivery System |
|---|---|---|---|
| Argon | Gas Laser | 488, 515 nm | Optical Fiber |
| KTP | Solid State | 532 nm | Optical Fiber |
| Helium–Neon (He–Ne) | Gas Laser | 633 nm | Optical Fiber |
| Diode | Semiconductor | 635, 670, 810, 830, 980 nm | Optical Fiber |
| Nd:YAG | Solid State | 1064 nm | Optical Fiber |
| Er, Cr:YSGG | Solid State | 2780 nm | Optical Fiber |
| Er:YAG | Solid State | 2940 nm | Optical Fiber, Waveguide, Articulated Arm |
| CO₂ | Gas Laser | 9600, 10600 nm | – (None specified / Direct Delivery) |
Laser Properties and Mechanism
The wavelength and properties of a laser depend mainly on the composition of its active medium, which can be a gas, crystal, or solid-state semiconductor.
Laser light can interact with target tissue in four different ways:
Reflection: The light returns to the source.
Transmission: The light passes through the tissue.
Scattering: The light is scattered in different directions.
Absorption: The light is absorbed by the tissue and its energy causes thermal and chemical changes in the tissue.
[Figure 3].
When laser light is absorbed by the tissue, the temperature increases and, depending on the amount of water in the tissue, various effects occur:
Ablation: At a temperature of about 100°C, the water in the tissue turns into vapor, leading to the direct removal of a portion of the tissue.
Protein denaturation: When the temperature is between about 60°C and 100°C, proteins lose their natural shape and function, without the tissue vaporizing.
Carbonization: When the temperature is above 200°C, the tissue dries and burns, which is an undesirable result.
In order for the laser light to be absorbed, we need specific light absorbers or chromophores, each of which is sensitive to specific wavelengths of light.
In the soft tissue of the mouth: melanin, hemoglobin and water are the most important chromophores.
In the hard tissue of the tooth: water and hydroxyapatite play the main role.
Each laser wavelength has a different absorption rate in these materials, so the choice of the type of laser is made depending on the type of tissue and the treatment goal.
Depending on the type of tissue, the application of lasers in dentistry is divided into two categories:
Application in soft tissue
Application in hard tissue
Laser applications in soft tissue
1. Aesthetic gingival remodeling and crown lengthening
With the advent of the diode laser, many specialists have made gingival esthetics part of their comprehensive orthodontic treatment [52,53]. Unlike traditional gingivectomy, which is associated with pain, bleeding, and discomfort, laser offers a more precise and comfortable procedure, improving the patient experience.
2. Exposure of impacted or partially erupted teeth
An impacted or partially erupted tooth can be exposed by conservative tissue resection, allowing for the placement of a bracket or button [Figure 5]. This procedure is performed without bleeding or pain and allows immediate bonding of the attachments.
3. Removal of inflamed or hypertrophic tissue
Small areas of excess or hypertrophic tissue can be easily removed with the diode laser, without the need for referral to a specialist [Figure 6]. This laser is also used to remove excess tissue over miniscrews, springs, and orthodontic appliances [Figure 7] and can replace traditional methods such as tissue punching [Figure 7].
4. Frenectomies
High or prominent lip frenum [Figure 8] as well as a shortened lingual frenum (ankylosglossia) [Figure 8] can cause swallowing, speech, malocclusion, and periodontal health problems. Laser frenectomy provides a minimally invasive and effective method to correct these problems, without pain, bleeding, or the need for sutures.
5. Wound healing
Low-level lasers stimulate cell growth and proliferation at low doses, such as 2 (J/cm²), but have a suppressive effect at high doses, such as 16 (J/cm²) [23,24].
This method affects the development and movement of fibroblasts, increasing the strength of healed wounds [25,26].
Studies have shown that low-level laser therapy (LLLT) can convert gingival fibroblasts into myofibroblasts, cells that are involved in wound contraction, and this effect is visible even 24 hours after treatment [27].
Positive effects of LLLT on the healing of aphthous lesions, post-pulpotomy dentinogenesis, mucositis, and oropharyngeal ulcers in patients undergoing radiotherapy have also been documented [28–30].
6. Herpetic lesions and aphthous ulcers
Photostimulation of aphthous and herpetic lesions with low-dose laser (HeNe) can reduce pain and accelerate the healing process [31–35].
In the case of herpes simplex labialis, photostimulation applied in the early stage can prevent the formation of painful blisters, reduce the overall healing time, and reduce the recurrence rate of lesions [36].
7. Disinfection using photoactivated dyes (PAD)
Low-level laser energy is able to activate photoactivated dyes and cause damage to the membranes and DNA of microorganisms.
PAD with a low-level diode laser (100 mW) and toluene chloride dye is highly effective in killing bacteria in subgingival plaque and resistant biofilms [37–39]. By using single-sided antibodies, PAD can be targeted and species-specific [40].
This method is able to kill gram-positive bacteria (including MRSA), gram-negative bacteria, fungi and viruses [41,42] and its main applications include the disinfection of root canals, periodontal pockets, deep carious lesions and peri-implantitis sites [43,44]. Tolunium chloride is also used in high concentrations for screening for oral and oropharyngeal mucosal malignancies [45,46].
8. Photodynamic therapy (PDT) for malignancies
PDT operates on the same principle as PAD and produces reactive oxygen species that damage cells and associated blood vessels, leading to necrosis and apoptosis [47].
This process also activates the host immune response and induces antitumor immunity [48]. Evidence suggests that PDT can stimulate the production of tumor necrosis factor alpha (TNF-α) [49]. Clinical studies have reported that PDT has been successful for carcinoma in situ and oral squamous cell carcinoma with a response rate of approximately 90% [50,51].
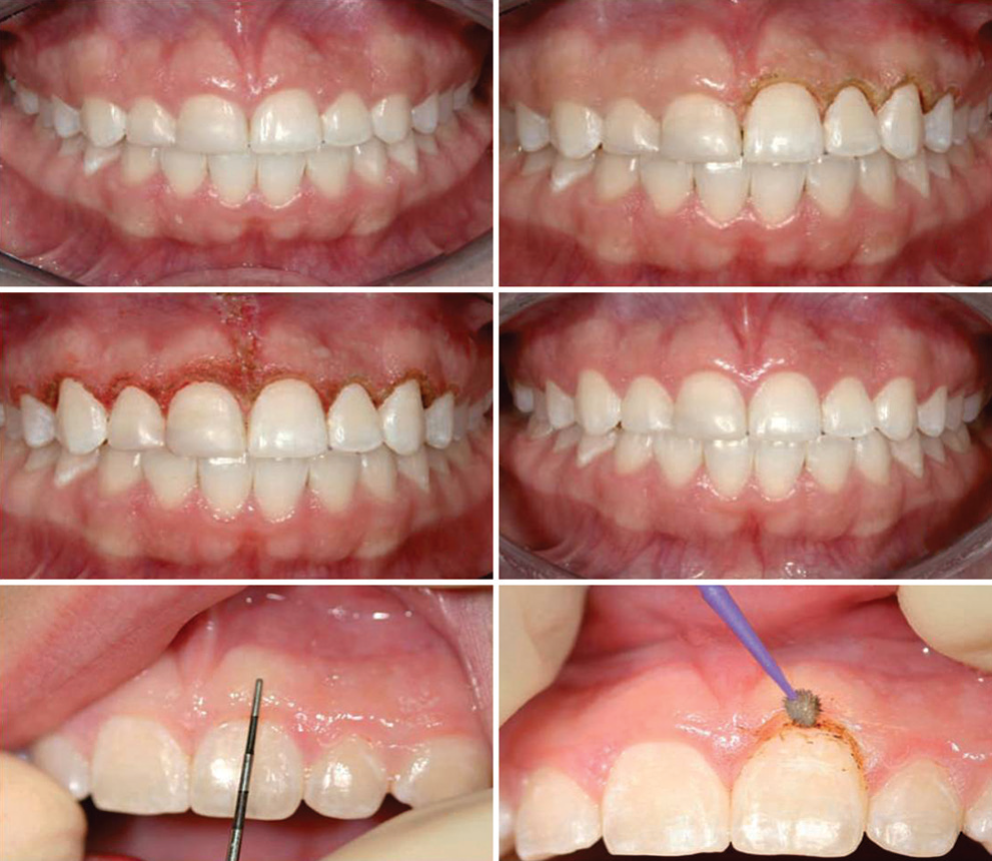
Figure 4: Aesthetic Gingival Contouring

Figure 5: Crown Exposure
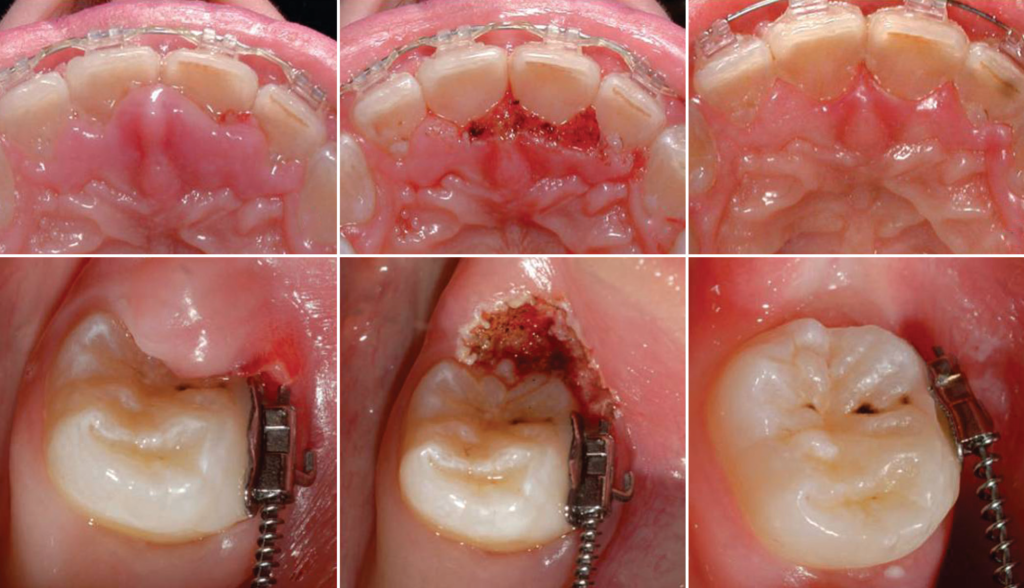
Figure 6: Hypertrophic Tissue Removal

Figure 7: Exposure of the coil placed during the traction procedure; creation of a punch hole for implant placement.

Figure 8: Upper lip frenectomy; and tongue frenectomy
Laser Applications in Hard Tissue
1. Photochemical Effects
The argon laser produces high-intensity blue light (488 nm) that is capable of initiating the photopolymerization process of photosensitive restorative materials in teeth, which use camphoroquinone as a photoactivator [54].
The argon laser beam can also alter the surface chemistry of the enamel and dentin [55], thereby reducing the likelihood of caries recurrence.
The bleaching effect of this laser is based on the absorption of green light with a wavelength of 510–540 nm by chelating compounds between apatites, porphyrins, and tetracycline compounds [56].
Argon and KTP (potassium titanyl phosphate) lasers can produce effective results in cases that do not respond to traditional thermal bleaching.
2. Laser fluorescence
Demineralization of enamel and the formation of white spots on the outer surface of teeth is a common side effect of fixed orthodontics [57,58]. However, evidence suggests that these small areas of enamel may remineralize [59].
3. Cavity preparation, caries removal, and restoration removal
Since 1988, the Er:YAG laser has been used to remove caries in enamel and dentin through supercavitation, without increasing the temperature of the dental pulp [60] and even without the need for water cooling [61]. This low-dose laser (LLLT) has a similar performance to air drills, except that the cavity floor is slightly rougher [62].
The Er:YAG laser can also remove cement, composite resin, and glass ionomer [63].
4. Laser etching
Laser etching has been investigated as an alternative to acid etching of enamel and dentin. Tooth surfaces etched with the Er, Cr:YSGG laser have surface microasperities and are free of smear layers [64]. However, the adhesion of restorations to the tooth after etching with Er:YAG is less than that after traditional acid etching [65,66].
5. Treatment of dentin hypersensitivity
Dentin hypersensitivity is one of the most common complaints in dental clinics. A comparison of the effects of the Er:YAG laser with traditional systems on sensitized dentin showed that this laser was effective in reducing dentin sensitivity and its effect lasted longer [67].
6. Diagnostic application
Lasers are used for diagnostic and research purposes in dentistry [Tables 2 and 3].
7. 3D scanner for electronic model preparation
Our understanding of the development of facial and cranial structures has improved with the development of accurate and low-cost 3D imaging systems. These systems can be destructive or non-destructive, for hard or soft tissue, and contact or non-contact [68-70].
The laser scanner can also be used as a soft tissue scanner and is a valuable tool due to its ease of use and the production of 3D images of dental structures. With this method, there is no need to prepare a physical mold, and electronic models are created directly from the mold impression.
These images are used to create a database of normal populations, to study growth changes, and to evaluate the clinical outcomes of surgical and nonsurgical treatments in the head and neck region [71-77].
Miscellaneous laser applications
1. Laser analgesic effect
Animal studies have shown that low-level laser therapy (LLLT) affects the nerves innervating the mouth and reduces the frequency of nociceptor activity. This effect has a threshold; that is, a certain intensity of radiation is required to achieve the maximum analgesic effect [78].
It has been reported that effective analgesic effects can be achieved after oral surgeries using all the main LLLT wavelengths from 632 to 904 nm [79,80].
Local CO2 laser irradiation can also reduce pain caused by orthodontic forces, without affecting tooth movement [81,82].
2. Nerve repair and regeneration
Studies have shown that low-level laser can reduce the production of inflammatory factors of the arachidonic acid family in injured nerves and enhance nerve growth and regeneration after injury [83,84].
LLLT protocols usually involve daily irradiation for long periods; for example, 10 days at a dose of 4.5 J/day [83].
Direct use of this method in dentistry has shown positive results in the regeneration of the inferior dental nerve (IDN) damaged during surgery.
3. Postoperative pain
A single session of LLLT at a dose of 0.9 to 2.7 J was 100% effective in reducing pain caused by apical periodontitis after root canal treatment and pain after tooth extraction [85].
However, results regarding pain reduction after tooth extraction with LLLT compared to a placebo control group have been reported to be mixed and sometimes contradictory [86-88].
Table 2: Diagnostic applications of lasers in the dental office
| Laser Type | Wavelength | Applications |
|---|---|---|
| Argon (Ar) | 488 nm | ✔ Detection of dental caries using laser fluorescence<br>✔ Laser Doppler fluorescence for evaluation of pulpal blood flow |
| Helium–Neon (He–Ne) | 633 nm | ✔ Scanning of phosphor plate digital radiographs<br>✔ Scanning of conventional radiographs for teleradiology |
| Diode | 633 nm | ✔ Laser Doppler flowmetry for pulpal blood flow measurement |
| Diode | 655 nm | ✔ Detection of dental caries using laser fluorescence<br>✔ Detection of subgingival calculus using laser fluorescence (porphyrin)<br>✔ Laser Doppler flowmetry for pulpal blood flow measurement |
| CO₂ | 10600 nm | ✔ Detection of fissure carious lesions through optical changes |
Table 3: Diagnostic applications of lasers as research tools in dentistry
| Laser Type | Wavelength | Applications |
|---|---|---|
| Nd:YAG | 1064 nm | ✔ Analysis of tooth structure using Raman spectroscopy<br>✔ Terahertz imaging of internal dental structures<br>✔ Spectroscopic decomposition analysis of dental material |
| Er:YAG | 2964 nm | ✔ Spectroscopic decomposition analysis of dental material |
| Argon | 488 nm and 515 nm | ✔ Confocal microscopic imaging of soft and hard tissues<br>✔ Flow cytometry analysis and cell separation |
| Helium–Neon (He–Ne) | 633 nm | ✔ Profilometry of dental surfaces and restorations |
| Diode | 633 nm and 670 nm | ✔ Profilometry of dental surfaces and restorations |
Sinusitis and Orthodontic Laser Applications
1. Sinusitis
The results of studies on the effectiveness of laser therapy for sinusitis are conflicting. One study [89] showed no significant benefit, while others reported that LLLT improved microcirculation, reduced swelling or fluid accumulation in the sinus area, and reduced the frequency of relapses [90].
2. Control of mandibular condylar overgrowth
Recently, diode lasers have been used in laboratory animals to control mandibular condylar overgrowth. Results showed that lasers can regulate facial growth and replace traditional methods such as chin-cups [91].
3. Effect of orthodontic forces on pulpal blood flow
McDonald and Pittford observed that pulpal blood flow in human teeth was reduced when continuous light forces were applied to maxillary canines [92].
Barwick and Ramsey used laser Doppler flowmetry to examine the effect of a four-minute orthodontic compressive force on pulpal blood flow and concluded that pulpal blood flow did not change during short-term compressive force applications [93].
4. Stimulation of bone formation and tooth movement
Recent studies have shown that low-energy laser irradiation can stimulate bone formation in vitro and in vivo.
Macrophage colony-stimulating factor (M-CSF) is necessary and sufficient for osteoclast formation.
Low-energy laser irradiation increases the rate of tooth movement by increasing M-CSF expression [94].
Laser safety in dentistry
Although most dental lasers are relatively simple to use, safety precautions are essential to ensure that they operate safely and effectively [95].
1. Eye protection
The most important consideration is the use of protective eyewear specific to the wavelength of the laser for all personnel present. This includes:
Dentist
Chairside assistants
Patient
Any other observers such as family members or friends
2. Environmental safety measures
Limit access to the surgical area
Reduce reflective surfaces
Ensure proper laser operation and review all manufacturer’s safety measures
3. Prevent transmission of infection
When hyperthermia is performed, high volume suction should be used to remove fumes and vapors.
Regular decontamination protocols should be followed.
4. Laser Safety Officer
Each clinic should have a Laser Safety Officer to:
Monitor proper use of the laser
Coordinate staff training
Monitor the use of protective eyewear
Be familiar with regulations related to laser safety
Medicolegal Considerations
Conservative laser surgery on soft tissue is within the scope of accepted dental practice and is usually covered by dental professional liability insurance.
Informed consent should always be obtained and is best done in the form of a general consent form that is read and signed by all patients before starting treatment.
Dentists are advised to take accredited laser training courses to fully master the operation of the device and safety precautions.
5. Prevention of contact with non-target tissues
The use of warning signs in the surgical environment can prevent laser radiation to non-target tissues
Conclusion
Laser technology in dentistry, both for hard tissue applications and soft tissue surgery, has reached a high level of development and advancement. Decades of research and development have shown that the use of lasers can significantly increase the accuracy, efficiency and comfort of dental treatments, and there is still room for further improvements.
Among the different types of lasers, the diode laser has become one of the most widely used and popular tools in clinical treatments due to its compactness, lower cost, ease of use and biostimulatory effects. This type of laser is not only effective for soft tissue surgery and removal of inflamed or hypertrophic tissues, but also plays a prominent role in pain relief, wound healing, nerve stimulation, and inflammation control.
The field of laser-based photochemical reactions, especially in combination with a diode laser of the appropriate wavelength, allows for precise targeting of cells, pathogens, and specific molecules, and therefore has great potential for novel therapeutic and diagnostic applications.
Furthermore, the combination of diagnostic and therapeutic techniques with lasers, especially with diode lasers, can enable early detection of oral and dental problems and targeted treatment with minimal damage to healthy tissue.
Looking to the future, it is predicted that the diode laser and related technologies will become an indispensable and inseparable tool in modern dentistry in the next decade and will play a vital role in increasing the quality, safety, and convenience of treatments.
References
- Maiman TH. Stimulated optical radiation in ruby lasers. Nature 1960;187:493.
- Walsh LJ. Dental lasers: Some basic principles. Postgrad Dent 1994;4:26‑9.
- Pick RM, Miserendino LJ. Lasers in dentistry. Chicago: Quintessence; 1995. p. 17‑25.
- Goldman L, Goldman B, Van‑Lieu N. Current laser dentistry. Lasers Surg Med 1987;6:559‑62.
- Frentzen M, Koort HJ. Lasers in dentistry: New possibilities with advancing laser technology. Int Dent J 1990;40:323‑32.
- Aoki A, Ando Y, Watanabe H, Ishikawa I. In vitro studies on laser scaling of sub‑gingival calculus with an erbium: YAG laser. J Periodontal 1994;65:1097‑106.
- Pelagalli J, Gimbel CB, Hansen RT, Swett A, Winn II DW. Investigational study of the use of Er: YAG Laser versus dental drill for caries removal and cavity preparation – Phase I. J Clin Laser Med Surg 1997;15:109‑15
- Walsh LJ. The current status of laser applications in dentistry. Aust Dent J 2003;48:146‑55.
- Einstein A. Zur Quantentheorie der Strahlung. Physiol Z 1917;18:121‑8.
- Gross AJ, Hermann TR. History of lasers. World J Urol 2007;25:217‑20.
- Fujiyama K, Deguchi T, Murakami T, Fujii A, Kushima K, Takano‑Yamamoto T. Clinical effect of CO2 laser in reducing pain in orthodontics. Angle Orthod 2008;78:299‑303.
- Fornaini C, Rocca JP, Bertrand MF, Merigo E, Nammour S, Vescovi P. Nd: YAG and diode lasers in the surgical management of soft tissues related to orthodontic treatment. Photomed Laser Surg 2007;25:381‑92.
- Aoki A, Mizutani K, Takasaki AA, Sasaki KM, Nagai S, Schwarz F, et al. Current status of clinical laser applications in periodontal therapy. Gen Dent 2008;56:674‑87.
- Slot DE, Kranendonk AA, Paraskevas S, Van der Weijden F. The effect of a pulsed Nd: YAG laser in non‑surgical perdiodontal therapy. J Periodont 2009;80:1041‑56.
- Harashima T, Kinoshita J, Kimura Y, Brugnera A, Zanin F, Pecora JD, et al. Morphological comparative study on ablation of dental hard tissue at cavity preparation by Er: YAG and Er, CR: YSGG lasers. Photomed Laser Surg 2005;23:52‑5.
- Ishikawa I, Aoki A, Takasaki AA. Clinical application of erbium: YAG Laser in periodontology. J Int Acad Periodontol 2008;10:22‑30.
- Hilgers JJ, Tracey SG. Clinical uses of diode lasers in orthodontics. J Clin Orthod 2004;38:266‑73.
- Carroll L, Humphreys TR. Laser‑tissue interactions. Clin Dermatol 2006;24:2‑7.
- Sulieman M. An overview of the use of lasers in general dentist practice: Laser physics and tissue interactions. Dent Update 2005;32:228‑30, 233‑4, 236.
- Sulieman M. An overview of the use of lasers in general dentist practice, laser wavelengths, soft and hard tissue clinical applications. Dent Update 2005;32:286‑8, 291‑4, 296.
- Tracey SG. Light work. Orthod Products 2005:88-93.
- Weiner GP. Laser dentistry practice management. Dent Clin North Am 2004;48:1105‑26.
- Tominaga R. Effects of He‑Ne laser irradiation on fibroblasts derived from scar tissue of rat palatal mucosa. Kokubyo Gakka Zasshi 1990;57:580‑94.
- Loevschall H, Arenholtd‑Bindslev D. Effect of low level diode laser irradiation of human oral mucosa fibroblasts in vitro. Lasers Surg Med 1994;14:347‑54.
- Noble PB, Shields ED, Blecher PD, Bentley KC. Locomotory characteristics of fibroblasts within a three‑dimensional collagenlattice: Modulation by a helium/neon soft laser. Lasers Surg Med 1992;12:669‑74.
- Asencio Arana F, Garcia FV, Molina Andreu E, Vidal MJ, Martinez SF. Endoscopic enhancement of the healing of high risk colon anastomoses by low‑power helium‑neon laser. An experimental study. Dis Colon Rectum 1992;35:568‑73. 27. Pourreau‑Schneider N, Ahmed A, Soudry M, Jacquemier J, Kopp F, Franquin JC, et al. Helium‑neon laser treatment transforms fibroblasts into myofibroblasts. Am J Pathol 1990;137:171‑8.
- Neiburger EJ. The effect of low‑power lasers on intraoral wound healing. NY State Dent J 1995;61:40‑3.
- Kurumada F. A study on the application of Ga‑As semiconductor laser to endodontics. The effects of laser irradiation on the activation of inflammatory cells and the vital pulpotomy. Ohu Daigaku Shigakushi 1990;17:233‑44.
- Kitsmaniuk ZD, Demochko VB, Popovich VI. The use of low energy lasers for preventing and treating postoperative and radiation‑induced complications in patients with head and neck tumors. Vopr Onkol 1992;38:980‑6.
- Iijima K, Shimoyama N, Shimoyama M, Yamamoto T, Shimizu T, Mizuguchi T. Effect of repeated irradiation of low‑power He‑ Ne laser in pain relief from postherpetic neuralgia. Clin J Pain 1989;5:271‑4.
- Olivi G, Genovese MD, Caprioglio C. Evidence‑based dentistry on laser paediatric dentistry. Eur J Paediatr Dent 2009;10:29‑40
- Yeh S, Jain K, Andreana S. Using a diode laser to uncover dental implants in second‑stage surgery. Gen Dent 2005;53:414‑7.
- Posten W, Wrone DA, Dover JS, Arndt KA, Silapunt S, Alam M. Low‑level laser therapy for wound healing: Mechanism and efficacy. Dermatol Surg 2005;31:334‑40.
- Ross G, Ross A. Low level lasers in dentistry. Gen Dent 2008;56:629‑34.
- Hargate G. A randomized double‑blind study comparing the effect of 1072‑nm light against placebo for the treatment of herpes labialis. Clin Exp Dermatol 2006;31:638‑41.
- Dobson J, Wilson M. Sensitization of oral bacteria in biofilms to killing by light from a low‑power laser. Arch Oral Biol 1992;37:883‑7.
- Sarker S, Wilson M. Lethal photosensitization of bacteria in subgingival plaque from patients with chronic periodontitis. J Periodontal Res 1993;28:204‑10.
- Wilson M. Bacterial effect of laser light and its potential use in the treatment of plaque‑related diseases. Int Dent J 1994;44:181‑9.
- Bhatti M, MacRobert A, Henderson B, Shepherd P, Cridland J, Wilson M. Antibody‑targeted lethal photosensitization of Porphyromonasgingivalis. Antimicrob Agents Chemother 2000;44:2615‑8.
- O’Neill JF, Hope CK, Wilson M. Oral bacteria in multi‑species biofilms can be killed by red light in the presence of toluidine blue. Lasers Surg Med 2002;31:86‑90.
- Seal GJ, Ng YL, Spratt D, Bhatti M, Gulabivala K. An in vitro comparison of the bactericidal efficacy of lethal photosensitization or sodium hyphochlorite irrigation on Streptococcus intermedius biofilm in root canals. Int Endodont J 2002;35:268‑74.
- Walsh LJ. The current status of low level laser therapy in dentistry. Part 2. Hard tissue applications. Aust Dent J 1997;42:302‑6.
- Dortbudak O, Haas R, Bernhart T, Mailath‑Pokorny G. Lethal photosensitization for decontamination of implant surfaces in the treatment of peri‑implantitis. Clin Oral Implants Res 2001;12:104‑8.
- Epstein JB, Oakley C, Millner A, Emerton S, van der Meij E, Le N. The utility of toluidine blue application as a diagnostic aid in patients previously treated for upper oropharyngeal carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;83:537‑47.
- Feaver GP, Morrison T, Humphris G. A study to determine the acceptability in patients and dentists of toluidine blue in screening for oral cancer. Prim Dent Care 1999;6:45‑50.
- Dougherty TJ. An update on photodynamic therapy applications. J Clin Laser Med Surg 2002;20:3‑7.
- Walsh LJ. Safety issues relating to the use of hydrogen peroxide in dentistry. Aust Dent J 2000;45:257‑69.
- Vowels BR, Cassin M, Boufal MH, Walsh LJ, Rook AH. Extracorporeal photophoresis induces the production of tumor necrosis factor‑alpha by monocytes: Implications for the treatment of cutaneous T‑cell lymphoma and systemic sclerosis. J Invest Dermatol 1992;98:686‑92.
- Fan KF, Hopper C, Speight PM, Buonaccorsi GA, Bown SG. Photodynamic therapy using mTHPC for malignant disease in the oral cavity. Int J Cancer 1997;73:25‑32.
- Biel MA. Photodynamic therapy and the treatment of head and neck neoplasia. Laryngoscope 1998;108:1259‑68.
- Sarver DM, Yanosky M. Principles of cosmetic dentistry in orthodontics: Part 2. Soft tissue laser technology and cosmetic gingival contouring. Am J Orthod Dentofac Orthop 2005;127:85‑90.
- Sarver DM, Yanosky M. Principles of cosmetic dentistry in orthodontics: Part 3. Laser treatments for tooth eruption and soft tissue problems. Am J Orthod Dentofac Orthop 2005;127:262‑4.
- Fleming MG, Maillet WA. Photopolymerization of composite resin using the argon laser. J Can Dent Assoc 1999;65:447‑50.
- Westerman G, Hicks J, Flaitz C. Argon laser curing of fluoride releasing pit and fissure sealant: In vitro caries development. ASDC J Dent Child 2000;67:385‑90.
- Lin LC, Pitts DL, Burgess LW. An investigation into the feasibility of photobleaching tetracycline‑stained teeth. J Endod 1988;14:293‑9
- Wisth PJ, Nord A. Caries experience in orthodontically treated individuals. Angle Orthod 1977;47:59‑64.
- Gorelick L, Geiger A, Gwinnett AJ. Incidence of white spot formation after bonding and banding. Am J Orthod 1982;81:93‑8.
- Marcusson A, Norevall L‑I, Persson M. White spot reduction when using glass ionomer cement for bonding in orthodontics: A longitudinal and comparative study. Eur J Orthod 1997;19:233‑42.
- Armengol V, Jean A, Marion D. Temperature rise during Er: YAG and Nd: YAP laser ablation of dentine. J Endod 2000;26:138‑41
- Burkes EJ, Hoke J, Gomes E, Wolbarsht M. Wet versus dry enamel ablation by Er: YAG laser. J Prosthet Dent 1992;67:847‑51.
- Cozean C, Arcoria CJ, Pelagalli J, Powell GL. Dentistry for the 21st century? Erbium: YAG laser for teeth. J Am Dent Assoc 1997;128:1080‑7.
- Dostalova T, Jelinkova H, Kucerova H, Krejsa O, Hamal K, Kubelka J, et al. Noncontact Er: YAG laser ablation: Clinical evaluation. J Clin Laser Med Surg 1998;16:273‑82.
- Hossain M, Nakamura Y, Yamada Y, Kimura Y, Matsumoto N, Matsumoto K. Effects of Er, Cr: YSGG laser irradiation in human enamel and dentin: ablation and morphological studies. J Clin Laser Med Surg 1999;17:155‑9.
- Martinez‑Insua A, Dominguez LS, Rivera FG, Santana‑Penin UA. Differences in bonding to acid‑etched or Er: YAG–laser–treated enamel and dentine surfaces. J Prosthet Dent 2000;84:280‑8.
- Ceballos L, Osorio R, Toledano M, Marshall GW. Microleakage of composite restorations after acid or Er: YAG laser cavity treatment. Dent Mater 2001;17:340‑6.
- Schwarz F, Arweiler N, Georg T, Reich E. Desensitising effects of an Er: YAG laser on hypersensitive dentine, a controlled, prospective clinical study. J Clin Periodont 2002;29:211‑5.
- Mah J, Hatcher D. Current status and future needs in craniofacial imaging. Orthod Craniofac Res 2003;6 Suppl 1:10‑6;179‑82.
- Quintero JC, Trosien A, Hatcher D, Kapila S. Craniofacial imaging in orthodontics: Historical perspective, current status, and future developments. Angle Orthod 1999;69:491‑506.
- Kau CH, Zhurov AI, Bibb R, Hunter L, Richmond S. The investigation of the changing facial appearance of identical twins employing a three‑dimensional imaging system. Orthod Craniofac Res 2005;8:85‑90.
- Yamada T, Mori Y, Katsuhiro M, Katsuaki M, Tsukamoto Y. Three‑dimensional analysis of facial morphology in normal Japanese children as control data for cleft surgery. Cleft Palate Craniofac J 2002;39:517‑26.
- Nute SJ, Moss JP. Three‑dimensional facial growth studied by optical surface scanning. J Orthod 2000;27:31‑8.
- Ayoub AF, Siebert P, Moos KF, Wray D, Urquhart C, Niblett TB. A vision‑based three‑dimensional capture system for maxillofacial assessment and surgical planning. Br J Oral Maxillofac Surg 1998;36:353‑7.
- Khambay B, Nebel JC, Bowman J, Walker F, Hadley DM, Ayoub A. 3D stereophotogrammetric image superimposition onto 3D CT scan images: The future of orthognathic surgery. A pilot study. Int J Adult Orthod Orthog Surg 2002;17:331‑41.
- Marmulla R, Hassfeld S, Luth T, Muhling J. Laser‑scan‑based navigation in cranio‑maxillofacial surgery. J Craniomaxillofac Surg 2003;31:267‑77.
- Moss JP, Ismail SF, Hennessy RJ. Three‑dimensional assessment of treatment outcomes on the face. Orthod Craniofac Res 2003;6 Suppl 1:126‑31; 179‑82.
- McDonagh S, Moss JP, Goodwin P, Lee RT. A prospective optical surface scanning and cephalometric assessment of the effect of functional appliances on the soft tissues. Eur J Orthod 2001;23:115‑26.
- Mezawa S, Iwata K, Naito K, Kamogawa H. The possible analgesic effect of soft‑laser irradiation on heat nociceptors in the cat tongue. Arch Oral Biol 1988;33:693‑4.
- Armida MM. Laser therapy and its applications in dentistry. Pract Odontol 1989;10:9‑16.
- Peres F, Felino A, Carvalho JF. Analgesic effect of 904‑nm laser radiation (IR) in oral surgery. Rev Port Estomatol Cir Maxilofac 1985;26:205‑17.
- Harazaki M, Isshiki Y. Soft laser irradiation effects on pain reduction in orthodontic treatment. Bull Tokyo Dent Coll 1997;38:291‑5.
- Turhani D, Scheriau M, Kapral D, Benesch T, Jonke E, Bantleon HP. Pain relief by single low‑level laser irradiation in orthodontic patients undergoing fixed appliance therapy. Am J Orthod Dentofacial Orthop 2006;130:371‑7.
- Mester AF, Snow JB, Shaman P. Photochemical effects of laser irradiation on neuritic outgrowth of olfactory neuroepithelial explants. Otolaryngol Head Neck Surg 1991;105:449‑56.
- Solomon A, Lavie V, Ben‑Bassat S, Belkin M, Schwartz M. New surgical approach to overcome the inability of injured mammalian axons to grow within their environment. J Neural Transplant Plast 1991;2:243‑8.
- Kawakami T, Ibaraki Y, Haraguchi K, Odachi H, Kawamura H, Kubota M, et al. The effectiveness of GaAlAs semiconductor laser treatment to decrease pain after irradiation. Higashi Nippon Shigaku Zasshi 1989;8:57‑62.
- Clokie C, Bentley KC, Head TW. The effects of the helium neon laser on postsurgical discomfort: A pilot study. J Can Dent Assoc 1991;57:584‑6.
- Fernando S, Hill CM, Walker R. A randomised double blind comparative study of low level laser therapy following surgical extraction of lower third molar teeth. Br J Oral Maxillofac Surg 1993;31:170‑2.
- Roynesdal AK, Bjornland T, Barkvoll P, Haanaes HR. The effect of soft‑laser application on postoperative pain and swelling. A double‑blind, crossover study. Int J Oral Maxillofac Surg 1993;22:242‑5.
- Moustsen PA, Vinter N, Aas Andersen L, Kragstrup J. Laser treatment of sinusitis in general practice assessed by a doubleblind controlled study. Ugeskr Laeger 1991;153:2232‑4.
- Kruchinina I, Feniksova LV, Rybalkin SV, Pekli FF. Therapeutic effect of helium‑neon laser on microcirculation of nasal mucosa in children with acute and chronic maxillary sinusitis as measured by conjunctival biomicroscopy. Vestn Otorinolaringol 1991;3:26‑30.
- Kharsa MA, Kharsa A. Use of laser in controlling the growth of facial structures, –Laser‑Orthopedics. Orthod Cyberjournal : http://orthocj. com/2005/08/laser-controlling-growth-of-facial-structures-laserorthopedics/ [Last accessed on 5th April 2012].
- McDonald F, Pitt Ford TR. Blood flow changes in permanent maxillary canines during retraction. Eur J Orthod 1994;16:1‑9.
- Barwick PJ, Ramsay DS. Effect of brief intrusive force blood flow on human pulpal blood flow. Am J Orthod Dentofacial Orthop 1996;110:273‑9.
- Yamaguchi M, Fujita S, Yoshida T, Oikawa K, Utsunomiya T, Yamamoto H, et al. Low‑energy laser irradiation stimulates the tooth movement velocity via expression of M‑CSF and c‑fms. Orthod Waves 2007;66:139‑48.
- Parker S. Laser regulation and safety in general dental practice. Br Dent J 2007;202:523‑32.
